Los Angeles has a food insecurity problem and much of it is hiding in plain sight.
“We were a bit surprised,” says Haik Janoian, operations manager for the nonprofit Eisner Health, over initial findings about how widespread food insecurity is among its clients. In a recent survey of 30 patients at Eisner Health, 23 reported running out of food before the end of the month. “We knew our patients were having a hard time,” Janoian says, “but it’s more than we thought.” Eisner Health is a community health organization that serves downtown Los Angeles, South L.A., and San Fernando Valley residents, where some 32,000 low-income patients visit the Federally Qualified Health Center’s 19 clinics annually.
It’s not just an Eisner Health problem. According to the Los Angeles Regional Food Bank, as many as one in five Angelenos, or about two million people, are food insecure—a problem that the U.S. Department of Agriculture (USDA) defines as a lack of consistent access to enough food for an active, healthy life because of a lack of money, and other resources.
In fact, Los Angeles County is home to the largest population of food insecure people in the nation, according to the Los Angeles Food Policy Council. Nearly 30 percent of low-income people in Los Angeles struggle with not knowing where their next meal will come from. And while more than one million Los Angeles County residents participate in the federally-funded CalFresh Food nutrition assistance program (known nationally as the Supplemental Nutrition Assistance Program or SNAP, formerly known as food stamps) that represents only 66 percent of people who are eligible for nutrition assistance. And even many recipients of CalFresh Food still struggle to meet their monthly food needs.
Given the scale and scope of this predicament, L.A. health clinics serving low-income communities are attempting to identify which of their patients are impacted by food insecurity and looking for ways to help meet this pressing need. Innovations in this area include screening for food security; sharing resources with patients such as grocery gift cards and referrals to food pantries; hosting pop-up farmers markets; partnering with food assistance organizations; and creating “food pharmacies.”
Six Los Angeles clinics — Altamed Health Services Corporation (in partnership with Children’s Hospital of Los Angeles), APLA Health, Behavioral Health Services, Eisner Health, Los Angeles LGBT Center, and St. John’s Well Child & Family Center — are part of an 18-month learning community called Moving Clinics Upstream, a CCI program funded by Cedars-Sinai. Moving Clinics Upstream is designed to address top patient health concerns, specifically food and transportation insecurity, by going beyond the walls of the health center to assess these challenging problems to providing healthcare for the communities they serve.
The end goal for all these clinics is similar: To connect food insecure patients who are falling through the cracks with resources in the community so they don’t go hungry. Adds Janoian: “It’s shocking that in Los Angeles there are so many people without enough food or money that they often go to bed hungry.”
Six Clinics, Six Different Needs, Six Different Solutions
There’s no one blueprint for combatting food insecurity among a clinic population. Each of the Moving Clinics Upstream participants, for instance, are tackling this challenge by addressing the needs of different demographics, which require different approaches and potential solutions.
In 2020, the clinics will continue conducting patient focus groups, analyzing survey data, and testing and implementing food security ideas based on patient input. The clinics will also explore ways to partner with like-minded organizations.
Here’s a quick snapshot of what each participant is working on:
- Altamed Health/CHLA is screening patients for food insecurity, using the Hunger Vital Sign, a two-question food insecurity screening tool developed by the Nutrition and Obesity Network (NOPREN). It’s also piloting a grocery delivery service for 10 families who have very low food security to assess how this meets their nutrition needs. And it’s doing three-month follow ups with families that have participated in its Food Resources for Kids (FORK) program, which connects patients to sources of no- and low-cost healthy food. The clinicians want to understand barriers and challenges to attaining food security before expanding their programming.
- APLA Health already has a robust food pantry operation, which it is in the process of expanding to meet 100 percent of their clients’ recommended daily nutrition needs. APLA Health, which serves a mostly low-income HIV-positive population at three clinic sites, is also exploring using One Degree, a social service referral platform often called the Yelp of community services. It would also like to include a community garden component staffed by volunteers.
- Behavioral Health Services is implementing the Hunger Vital Sign screening tool at two clinic sites and will have specialized care coordinators use One Degree to make and track referrals at their Crenshaw clinic. BHS will collect data on the number of patients screened, the number of patients enrolled in CalFresh Food, and the number of referrals made to food resources. It also partnered with Wholesome Wave, offering $25 grocery gift cards to 1500 patients at three clinics as part of a pilot program. It is exploring the possibility of providing a ‘food prescription program’ and potentially hosting a pop-up farmers market on site.
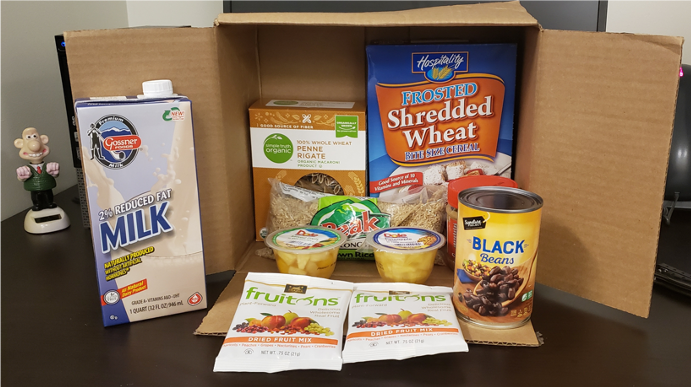
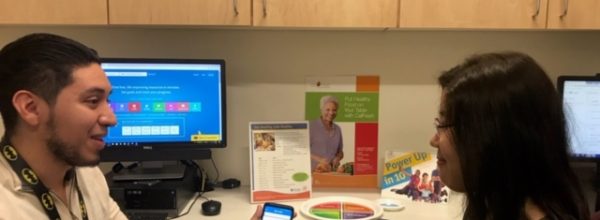
- Eisner Health is partnering with LA Neighborhood Land Trust and the L.A. Regional Food Bank on care packages distributed at its clinics as part of a pilot. Many families have expressed a preference to picking up groceries at the clinic. The clinic is also piloting talking tablets to survey patients about food insecurity.
- LA LGBT Center is screening patients for food insecurity using both the Hunger Vital Sign and survey tool PRAPARE (Protocol for Responding to and Assessing Patients’ Assets, Risks, and Experiences). It is also working on training staff to help patients sign up for CalFresh Food and distributing grocery gift cards. It is also exploring partnering with an organization to offer a food pantry on site.
- St. John’s Well Child & Family Center is getting ready to launch its own mobile food pantry, with the assistance of the L.A. Regional Food Bank, at its Crenshaw site. It is also referring food insecure patients to resources via the online tool Aunt Bertha.
What Food Insecurity Looks Like: The Big Picture
 Food insecurity is a widespread problem in the United States — it impacts seniors, immigrants, people of color, children, single-parent households, the unexpectedly unemployed, the working poor, the unhoused, college students, the LGBTQ+ community, urbanites, and rural residents. In 2018, an estimated 11 percent of American households were food insecure — that’s more than 37 million people, including 11 million children. Food insecurity can be chronic or temporary and can be impacted by neighborhood conditions. For instance, many low-income people in urban neighborhoods lack access to full-service supermarkets or grocery stores.
Food insecurity is a widespread problem in the United States — it impacts seniors, immigrants, people of color, children, single-parent households, the unexpectedly unemployed, the working poor, the unhoused, college students, the LGBTQ+ community, urbanites, and rural residents. In 2018, an estimated 11 percent of American households were food insecure — that’s more than 37 million people, including 11 million children. Food insecurity can be chronic or temporary and can be impacted by neighborhood conditions. For instance, many low-income people in urban neighborhoods lack access to full-service supermarkets or grocery stores.
The USDA divides food insecurity into two categories: Low food security people, who experience a reduction in the quality, variety, or desirability of their diet; and very low food security individuals, who have disrupted eating patterns, reduced food intake, and experience hunger. Adults who are food insecure may skip meals or buy unhealthy foods — full of fat, salt, or sugar — because they are often more affordable and accessible than nutritious ones, putting this population at greater risk for diabetes, high blood pressure, obesity, depression, and other health conditions, says Dr. Dipa Shah, director of the nutrition and physical activity program at the Los Angeles Department of Public Health, which is a resource on food insecurity assistance, research, and screening in L.A. Food insecure children are at greater risk for asthma, behavioral problems, impaired growth, obesity, and poor school performance, according to Shah.
The stigma many associate with not having enough food to eat means often food insecure people are reluctant to ask for assistance accessing nutritious food, which can be detrimental to physical, emotional, and mental health. Food insecurity — and its nutrition-related deficits — can exacerbate existing acute or chronic medical problems or cause nutrient-related health concerns. “Some of the patients who screened positive were people I’ve known for years. That was alarming,” says Eisner Health case worker Felix Dominguez. “I had no idea. They were too embarrassed to bring it up or they’re fearful because of their immigration status, or because of public charge, or a visit from CDSS [Child Protective Services].”
That sentiment is echoed by other health centers in the Moving Clinics Upstream cohort, currently in the information-gathering phase of teasing out both the extent of this problem and potential solutions to it among their clients.
The Many Contradictions of Food Insecurity
Paradoxes abound when it comes to food insecurity: It is largely an access and food distribution issue, versus a lack of available food, especially in California, with its farm-fresh abundance. L.A., once the largest agricultural county in the United States, is now the county with the largest population of food insecure people, according to an in-depth 2018 Global Citizen report on the complex problem. And there is a statistically higher level of prevalence of obesity among populations with a higher prevalence of food insecurity, according to the 2015 Los Angeles County Public Health report “Rising Food Insecurity in Los Angeles County.” In the United States it is possible to be both overfed and undernourished.
Food Insecurity isn’t a hunger problem, per se, it’s a poverty problem, according to experts in the area. In a region with a high cost of living—including housing and transportation—even two-income families earning well above minimum wage can find it a struggle to pay the bills and put sufficient, adequate food on the table for everyone in the home. Rents in Los Angeles County have increased by nearly one-third since 2000, according to a 2017 L.A. Weekly story on food insecurity. Families are making difficult choices about whether to pay for food or housing.
“At the heart of this work, I think we all face similar challenges in L.A. centered around access and competing priorities for many families,” says Amanda Daigle, program administrator for advocacy and education at Children’s Hospital Los Angeles. “Los Angeles is an incredibly expensive city for housing, which directly impacts a family’s ability to afford and access food. And given how spread out the city is, it can often be difficult for families to utilize public transportation to get to food resources or even grocery stores.”
While hunger refers to an individual physical sensation of discomfort due to a need for nourishment, food insecurity refers to a lack of access to nutritious food and a lack of money and other resources. And while food insecurity and poverty frequently coincide, not all people living below the poverty line experience food insecurity. In addition, people who aren’t considered poor can experience food insecurity.
“There is so much need out there for food assistance,” says Eisner Health’s Dominguez. “Once we’ve identified the problem, patients start opening up about the challenges they face. Our patient population is very grateful for the services we provide.” Eisner Health is currently focusing on food security among its pediatric patients—families with small children—with the goal to expand these services to all their patients in need.
Applying Design Thinking
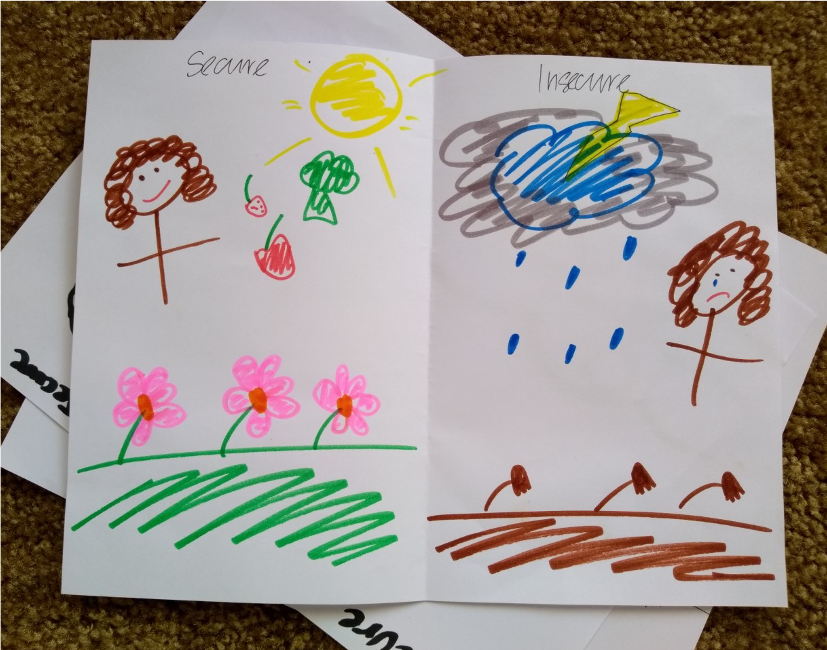
To get a handle on how food insecurity is impacting their clinics from their patients’ perspectives, Moving Clinics Upstream taught the Los Angeles clinics “design thinking” techniques such as open-ended interviews, draw your own experience exercises, and observation activities. This human-centered design approach to problem solving is collaborative, creative, and begins by understanding people’s needs and experiences.
The end goal is to find solutions to food insecurity; but right now, these clinics are reaching out to patients to understand the extent of the problem.
These design thinking activities uncovered a range of common themes—many patients reported sadness, fear, and shame about their food insecurity, according to clinic staffers, including Louis Guitron, director of case management services at the Los Angeles LGBT Center. And many conveyed just how critical these services and support are to help ward off hunger. One patient experiencing homelessness and mental health issues at St. John’s told clinic staff that when he is manic he doesn’t have the capacity to go to a food bank to find food.
Some preliminary findings reveal significant need:
- In a survey of 68 St. John’s Health Center patients (housed and unhoused) 38 said in the past 12 months they experienced food insecurity.
- In a survey at the Los Angeles LGBT Center, 12 out of 18 patients screened positive for food insecurity and 4 out of 18 were uncomfortable talking with staff about their food needs.
- In a focus group with seven food insecure families and a social work case manager, AltaMed/CHLA learned that barriers to accessing affordable food among patients includes concern around immigration status, stigma around accepting food bank or grocery gift card assistance, and lack of transportation.
Patients were candid about their struggles:
- “When I don’t have food that means I don’t have money as well. And that is all bad.”
- “There’s a lot of stress that goes into play when you’re worrying about not being able to feed yourself or your children.” – mother of two young daughters
- A food insecure patient talked about growing up in a family on food stamps—there was never enough to eat—and not realizing that not every family accessed food that way.
And the design thinking techniques helped to pinpoint underlying food insecurity concerns. “‘Draw your experience’ was useful in setting the tone for the focus group,” says Carolina Rodriguez Orozco, quality improvement coordinator, at Behavioral Health Services in Gardena. BHS is a not-for-profit community-based healthcare organization providing medical services, substance abuse, mental health, drug-free transitional living, housing for women with HIV, and prevention services for the local community at 21 clinic sites in Los Angeles County. “The focus groups enabled us to connect with our patients in a meaningful way. That’s how we were able to find out that our patients are still struggling with food insecurity despite having CalFresh.”
Food insecurity typically doesn’t stand alone. Often a patient screening positive for food insecurity has multiple other presenting social needs for housing, employment, education, immigration status, transport, or mental health. Clinic staff need assistance and training with helping patients prioritize addressing their needs.
“It’s vital to really talk to those on the ground: case managers and families themselves, whether through focus groups or draw your experiences,” says Daigle. “We feel that we cannot do this work in an impactful or sustainable way without involving community members in the co-creation of our strategies.”
Lessons From a Model Clinic
Earlier this year, representatives from the six clinics attended a site visit at the Northeast Valley Health Corporation (NEVHC), a Federally Qualified Health Center in Sylmar, L.A.’s most northern neighborhood located in the San Fernando Valley, to learn about its food insecurity screening tools, internal resources, external referrals, and community partnerships for these at-risk patients with nonprofit organizations such as MEND. (Read our case study about NEVHC to learn more.)
“It was helpful to witness a well-organized, well-resourced, well-staffed program at a health center with a strategic, sustainable, long-term view for addressing food insecure patients,” says Eisner’s Janoian.
Among the findings that the NEVHC team shared with this group:
- Training staff, including front office workers, medical assistants, volunteers, and promotoras (community health workers), on a standardized response to food insecurity screening alerts is key.
- Teaching staff how to guide patients, as needed, through the process of using technology tools is also important.
- Keeping in mind that staff and/or community liaisons themselves may be food insecure.
- Soliciting buy-in from all team members is crucial to adding food insecurity screening to an already full clinic visit.
- Inviting patients to share their food insecurity experiences and how screening for the condition helped them access food can have a marked impact on staff buy-in. These kinds of testimonials help staff connect the dots, showing how a screening can improve patients’ quality of life.
Technology Lends a Hand
Technology can help with efficiency when screening for food insecurity and other social needs and may result in a more honest response than a paper or in-person intake, the six clinic cohort learned on their site visit at NEVHC. Perhaps interacting with a computer tablet feels somehow more private than an encounter with a case worker.
But technology is not a substitute for human connection. Each patient has unique circumstances and challenges that may require a targeted and personal approach to assistance, NEVHC staff explained. Adequate training for health center staff is important to conduct compassionate, sensitive, effective food insecurity screening that is supportive, empathic, and non-threatening to patients. Little wonder then that this work is hard, time-consuming, and requires buy-in at multiple levels. Clinics have found that in many cases medical assistants, case workers, and promotoras need to assist patients with surveys (if, say literacy or language is an issue), or benefit applications (which can be daunting, regardless of literacy).
Meeting Patients Where They’re At: Culturally-Sensitive Care
As participants’ field trip to NEVHC made clear, it’s not enough to simply direct patients to resources — some pantries aren’t open convenient hours, or stock poor-quality food; some patients aren’t able to transport food or can’t find enough food at food pantries, or aren’t able to store food or don’t have access to a kitchen. For those patients who screen positive for further assessment, follow up by clinic staff or a community health worker is important to ensure that patients get the help they need.
Bringing food to the health-care setting — in the form of tote bags or boxes, a mobile pantry, or a pop-up produce market — is seen as a desirable workaround for patients who lack transit, or work during food pantry hours, or don’t have childcare. A pop-up produce market at a NEVHC clinic, in partnership with Cal Fresh Healthy Living, run by clinic staffers and patient volunteers is an example of an effort to fill the gap here. This “farmers market” style model of food assistance, where clients can choose food they’re familiar with and likely to eat and cook, encourages dignity and limits food waste.
During the NEVHC’s pilot program the organization held patient focus groups, which revealed that many patients were unfamiliar with the term “food pantry,” did not understand how food banks function, and some believed that eating food past sell-by dates was potentially dangerous. The team, which toured local food pantries, also learned that many of the available foods were unfamiliar to their patient population. To help patients understand resources available to them, the team developed a comprehensive educational Food Rx Guide that is accessible, healthy, and references culturally appropriate food and includes contacts for local food pantries (renamed “free groceries” for the purposes of clarity), meal plans, recipes, information on food labeling and safety, as well as details about NEVHC nutrition classes and programs. Care teams now hand the guide out during well-child visits.
NEVHC didn’t stop there. The team started offering monthly nutrition workshops, where they educated patients about available food resources and connected patients to food assistance programs such as CalFresh Food and WIC. It also hosted garden classes in its demonstration produce plot. “Getting to see how a pop-up market and garden can be incorporated into a health care setting was exciting,” says BHS’s Rodriguez Orozco. “NEVHC proves that with dedicated staff it is possible to do more to connect patients to food resources.”
One other consideration in this work: Patients may have an emotional response to seeking or accepting food assistance — which may differ from feelings around accepting help or subsidies for housing, utilities, or transit. Clinics need to keep this in mind when seeking solutions.
“Unless you’re behind the scenes, it’s really hard to understand just how tough it is out there,” says Eisner Health case worker Felix Dominguez. “We’re all working towards making sure our patients get the critical food assistance they need.”