Lack of Communication as a Barrier to Care
For the past 40 years, Santa Cruz Community Health Centers (SCCHC) has provided quality, affordable, comprehensive health care services — from primary care to acupuncture treatment — to 10,500 people in the city of Santa Cruz and the surrounding area. Many families who live in Live Oak, an unincorporated community near Santa Cruz, rely on SCCHC for medical care.
Live Oak has a large number of low-income residents: 57 percent of the students in the Live Oak School District are low-income, 54 percent are Latino, and as many as 25 percent of the students at one elementary school are homeless. Many students struggle academically: At Live Oak Elementary School, for example, only half of third grade students read at grade level.
SCCHC and Live Oak School District staff were frustrated that many of their high- risk, high-need students, who have complex health, family, and academic needs, weren’t showing much improvement. These young people often have multiple barriers to care, including poverty, social isolation, disorganized home environments, parental trauma and mental health issues, and illiteracy. These factors lead to decreased school attendance, missed clinic visits, and lack of follow through on care plans and academic remediation, all of which further prevent the children from getting the care they need.
SCCHC and school staff recognized yet another barrier to care: there was little communication between healthcare providers, teachers, and parents. As one SCCHC staff member put it, “Health providers were in the dark about how their patients were faring at school, educators were at wit’s end with their students’ complex health and family needs, and parents were disengaged, overwhelmed, or confused about how to support their high-need children.”
School and clinic staff alike recognized that this situation wasn’t serving the young people who were at highest risk, and they decided to do something about it.

To get started, staff at SCCHC and the Live Oak School District launched the Live Oak Community Care Team. To build and guide the Team, staff tapped into an existing resource: the Live Oak Cradle to Career Initiative (C2C). C2C was created by parents at the Live Oak Preschool and local health, education, and social service representatives to create an integrated support system for high need families. Since its founding four years earlier, C2C has helped build relationships between participating institutions, and these bonds helped build a strong foundation for the Community Care Team.
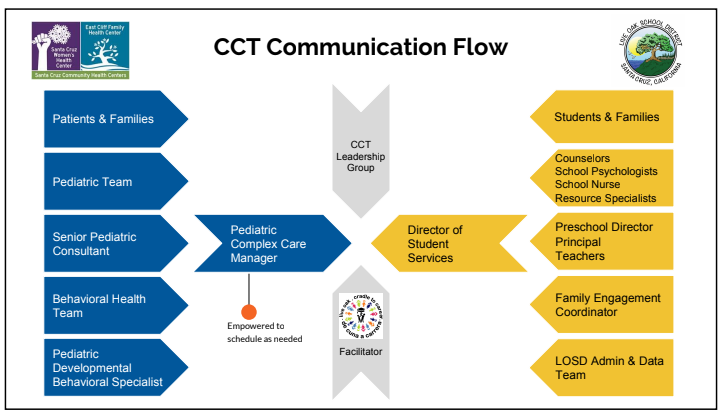
C2C’s Social Impact Consultant was brought on as the Community Care Team’s facilitator, and a Leadership Group was formed. The Leadership Group worked together to create a structure for the new group, and to decide goals and processes. They shared their plans with SCCHC and school district staff, who provided feedback and recommendations.
SCCHC obtained a grant from CCI, and subgranted monies to the Live Oak School District to solidify the partnership. The CCI grant was used to cover a percentage of clinical staff time, consultant hours, the subgrant to the school district (to supplement counseling and clinic staff time); a small portion was used for food and miscellaneous expenses. CCI also provided project support, coaching, and access to data, fundraising, and legal expertise.
The Leadership Group designed a plan for Community Care Team Case Conferences. The Case Conferences are meetings where an interdisciplinary group of health care providers, educators, and social service representatives gather to consider the cases of high-risk students, and formulate care plans. The Leadership Group created an agenda for the conferences, figured out the process for Release of Information (ROI), and created a conference evaluation form and a case tracking form (the latter proved hard to use and was later replaced with a simple spreadsheet.)

Case Conferences focus on one to two students (when two students’ cases are considered, the conferences are divided into two time slots, with the group discussing each student individually). First, the Community Care Team listens to a three-minute audio recording of the child’s parent. In the recordings, parents discusses their hopes and dreams for their child. Next, clinic and school representatives give their respective observations of the student, including family situation, health concerns, treatment and referrals, Individual Education Plans, school attendance, behavior, and other information. The group then works together to identify system-level solutions and to develop unified care plans. Staff are assigned follow-up tasks. (See Community Care Team Case Conference Agenda for more detail.)
The Community Care Team met monthly, holding a Case Conference and a Leadership Group Meeting in alternating months. The Leadership Group meetings provided the opportunity to plan conferences, follow-up on ongoing cases, refine the agenda, address data management issues, and regularly review and improve project goals and practices.