California is embarking on a shift in how it pays for health care. And with that shift in payment, there will also be a need to transform care processes and systems to better care for patients. But there’s a lot of unknowns about payment reform, what it is going to look like, when it’s going to happen. We recently encountered another setback with moving our alternative payment model (APM) forward through the proposed State Amendment Plan in California. However, what we’ve learned from our friends in Oregon and Colorado who have begun their APM is that regardless of the unknowns, care transformation is a process that takes time and we can’t wait for payment reform to make changes to the way we deliver care. We need to start testing and piloting changes NOW, so clinics can succeed in a value-based environment.
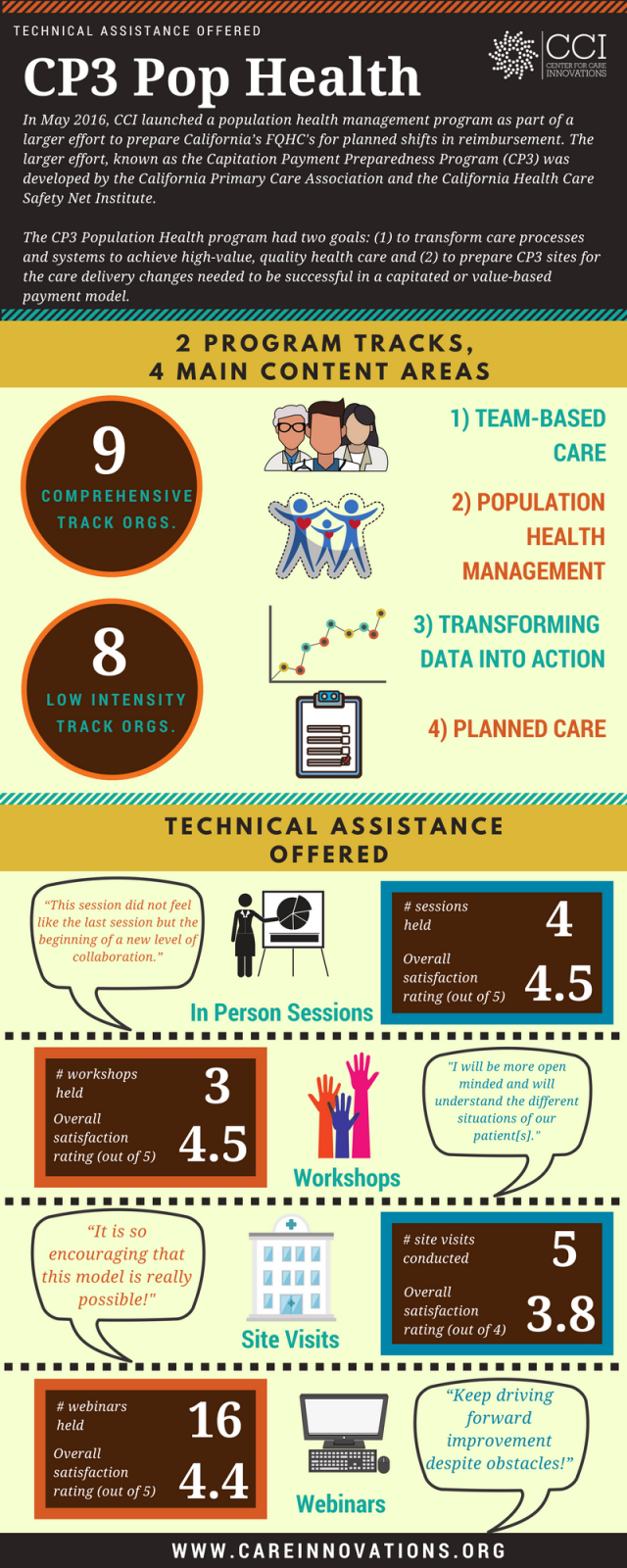
And that’s what we’ve been doing since June 2016 in the population health track of the larger Capitation Payment Preparedness Program (CP3): helping a cohort of clinics test out changes to the way they provide care. Our aim is to help organizations test changes in three core areas to support the delivery of high-value care in a capitated payment environment. Those three areas are team-based care, population health management, and planned care. And over the past year we’ve had a series of wins among our teams. They’ve been busy communicating and getting buy-in, building new foundations to do population health work, making changes to their care teams, and experimenting with alternative touches.
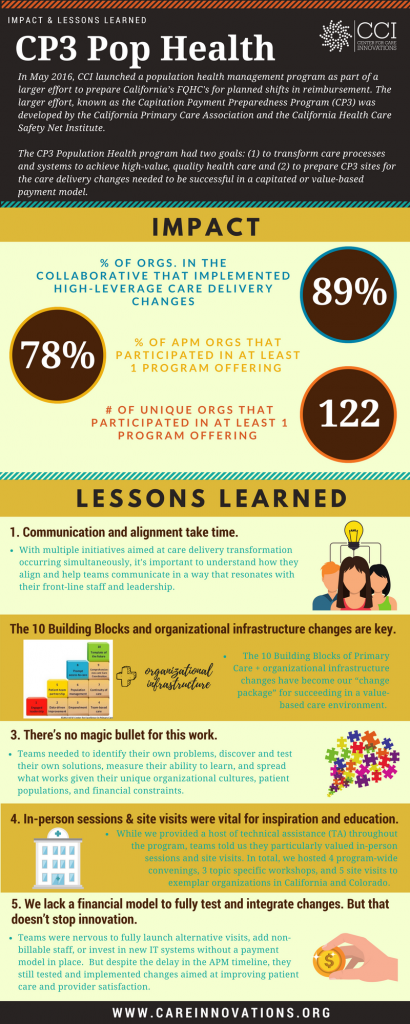
What worked for our teams? We want to share some insights, reflections, and recommendations that will inform our work moving forward:
1. Communication and alignment take time.
Organizations expressed confusion about the different care delivery transformation initiatives that exist, how they link together, and how best to communicate about CP3 in a way that resonates with their front-line staff. It was clear that organizations spent several months figuring out their engagement strategy to bring leadership and front-line staff on board. We spent time in the program on change management and leadership training, including content on creating an organizational vision, incorporating APM goals into overall strategic plans, developing improvement teams and clear roadmaps, and understanding adaptive leadership strategies.
We also spent time on communication planning: how to develop a plan that addresses the question “What’s in it for me?” at all levels of staff, formulating succinct elevator pitches, aligning the APM with other transformation initiatives, and recognizing and verbalizing “adaptive challenges” vs. “technical challenges” to leadership and front-line staff.
Teams needed to have an integrated approach, and this took longer and more time than we anticipated.
2. The 10 Building Blocks and organizational infrastructure changes are key.
Our program reinforced the importance of the 10 Building Blocks of High-Performing Primary Care. We spent time working on these foundational blocks, such as team-based care and empanelment, to help teams envision a future roadmap for providing care. But we also learned that organizations that want to succeed in a value-based care environment need to go above and beyond.
We learned that successful organizations focus on developing people, processes, and systems to provide quality care. These are proactive vs. reactive organizations. They have systems in place to understand their patients, identify care gaps, and provide care interventions at the right time, by the right person, and in the right way. They have knowledge management systems to capture and reinforce training. And they have mindsets geared toward improvement and innovation. The 10 building blocks in addition to these organizational infrastructure changes have become our “change package” for succeeding in a value-based care environment. You can learn more about our work by reading my colleague Tammy Fisher’s recent perspective piece.
3. There’s no magic bullet for this work.
We learned that there is no single solution. Teams needed to identify their own problems, discover and test their own solutions, measure their ability to learn, and spread what works given their unique organizational cultures, patient populations, and financial constraints.
As a result, projects covered a wide variety of issues. Some teams in the program spent a majority of their time making changes to their care teams, including testing out what roles and task are needed to support value-based care. Others focused on what data and roles are needed to support both in-reach and outreach activities. Many tested what alternative visit types are most appropriate for their patient population, including patient portals, shared medical appointments, and telephone visits.
4. In-person and site visits were vital for inspiration and education.
While we provided a host of technical assistance (TA) throughout the program, teams told us they particularly valued in-person convenings and site visits.
In total, we hosted four in-person convenings for Comprehensive Track participants and three daylong workshops geared toward Low Intensity Track participants. As teams tested and made changes, we learned it’s important to bring this community together to share lessons learned and discuss ideas. By the end, one participant shared “
Site visits to Petaluma Health Center, West County Health Centers, and Clinica Family Health, where teams could see firsthand the different ways that organizations have made changes, were key to inspiring team members and encouraging them to continue innovating. Teams reported learning ideas about how to ensure staff work at the top of their license; enhance data visualization; improve communication, including mandatory huddles and “cuddles”, Vocera badges, and email protocols; design care teams, including the role of spatial design, co-location and behavioral health integration; and create cultures around continuous learning. After a site visit, one participant remarked: “It is so encouraging that this model is really possible.”
5. We lack a financial model to fully test and integrate changes. But that doesn’t stop innovation.
And finally, we learned through the program that to move from prototyping to implementation, a new payment model is critical. Teams were nervous to fully launch alternative visits, add non-billable staff, or invest in new IT systems without a payment model in place.
At the same we saw that there is a lot of work that can be done in lieu of a new model. Given that we are living in unpredictable times, organizations were eager to figure out what changes they want and what they can do now to improve patient care and provider satisfaction, regardless of the larger political environment.
What key changes is your organization testing out to prepare to succeed in a value-based environment, and what challenges are you still encountering? As we move forward with planning additional programming, we’d love to hear from you what support you think is important to transform the way your organization delivers care.
INFOGRAPHICS: Click to enlarge