 Challenge
Challenge
Axis serves hundreds of patients seeking behavioral health care each week. However, the behavioral health department previously lacked the systematized and comprehensive access to data that other departments, such as primary care, have created and utilized. Despite using various tools to document behavioral health outcomes, tracking and monitoring patients’ depression, anxiety, and drug use over time had been difficult. The department’s main barrier was a lack of technology infrastructure to pull data and analyze it longitudinally – that is, to track trends in patient care and outcomes over time. Data is particularly important in population health management to identify which specific populations are receiving care, measure the outcomes, and adjust care accordingly. The inability to track patients often prolonged patients’ time in care and made it difficult for the team to evaluate treatment methods.
 “We lacked organization around the severity of our patient health, specifically for our patients who have depression. We didn’t have a means of tracking improvements over time and throughout treatment. Our therapists did not have automated or real-time reports on their panels, which made it difficult for them to review and act on in a timely manner.” – Afsheen Islam, Quality Enhancement Manager
“We lacked organization around the severity of our patient health, specifically for our patients who have depression. We didn’t have a means of tracking improvements over time and throughout treatment. Our therapists did not have automated or real-time reports on their panels, which made it difficult for them to review and act on in a timely manner.” – Afsheen Islam, Quality Enhancement Manager
 Goals
Goals
- Create a pilot study registry to track scores throughout treatment from the Patient Health Questionnaire-9 (PHQ-9) — a brief tool that screens for and measures the severity of a patient’s depression — and follow up by expanding the registry to include scores from screening tools that measure anxiety and drug use.
- Examine data through the registry to identify patients whose behavioral health scores were not improving.
- Adjust treatment as needed.
- Measure improvements.
Team
 Axis’ PHLN project team was led by the organization’s Quality Enhancement Manager and the Chief Quality and Transformation Officer, together with the Chief of Behavioral Health, who has encouraged and facilitated the creation of a data registry. In order to fulfill the goals of the project, they collaborated with members of the behavioral health team, which includes 19 licensed providers that see 500 to 600 patients a week, as well as a consulting psychiatrist and managing providers who help with medication dissemination.
Axis’ PHLN project team was led by the organization’s Quality Enhancement Manager and the Chief Quality and Transformation Officer, together with the Chief of Behavioral Health, who has encouraged and facilitated the creation of a data registry. In order to fulfill the goals of the project, they collaborated with members of the behavioral health team, which includes 19 licensed providers that see 500 to 600 patients a week, as well as a consulting psychiatrist and managing providers who help with medication dissemination.
 Key Changes
Key Changes
Axis created a system to engage behavioral health providers in using data to drive and improve outcomes among its patient population with behavioral health diagnoses. Through the PHLN, Axis developed a robust behavioral health registry within Epic that monitors and tracks key health indicators. Axis specifically tracks patients’ scores from the PHQ-9 (which screens for depression severity), Generalized Anxiety Disorder-7, or GAD-7 (which screens for generalized anxiety disorder and its severity), and the Drug Abuse Screening Tool, or DAST-10 (which screens for drug use and provides an index of the degree and types of problems that drug use has caused the patient). The registry equips providers to use this data to adjust treatment plans in a timely manner.
 Strategy
Strategy
1. Track Patient Scores
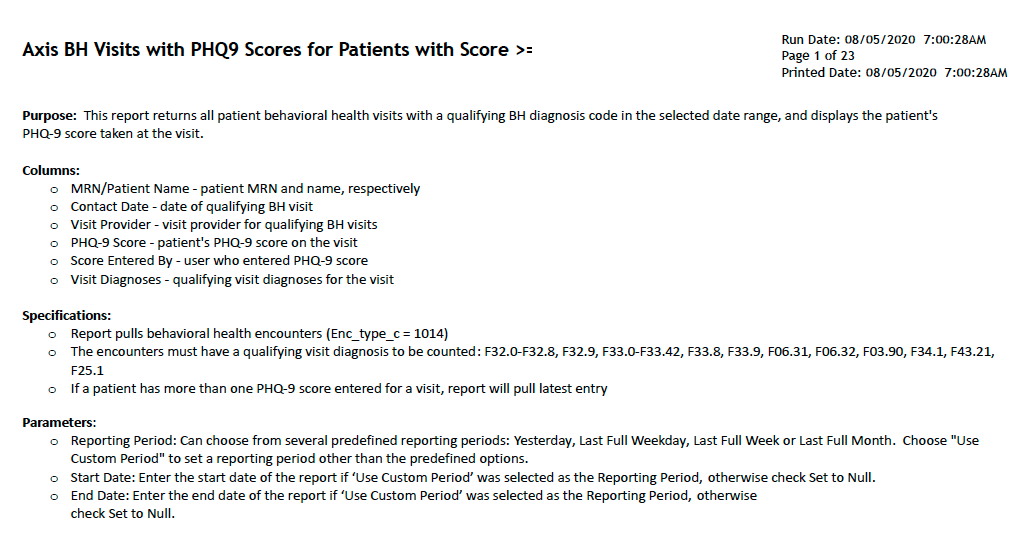
Patients are asked to complete the PHQ-9, GAD-7, and DAST screenings on a tablet when they arrive at the health center. When submitted, the data is automatically integrated into Epic. Using SQL, the standard query language used to communicate with a database, the team created a query that pulls key information into a behavioral health patient registry. The registry is comprised of the following information, which was initially tracked over a five-month period:
- Patient name
- Date of appointment
- Provider seen
- Current medications
- Screening Scores (initially just PHQ-9 in the pilot)
- Provider who entered screening scores
- ICD-10 diagnosis code
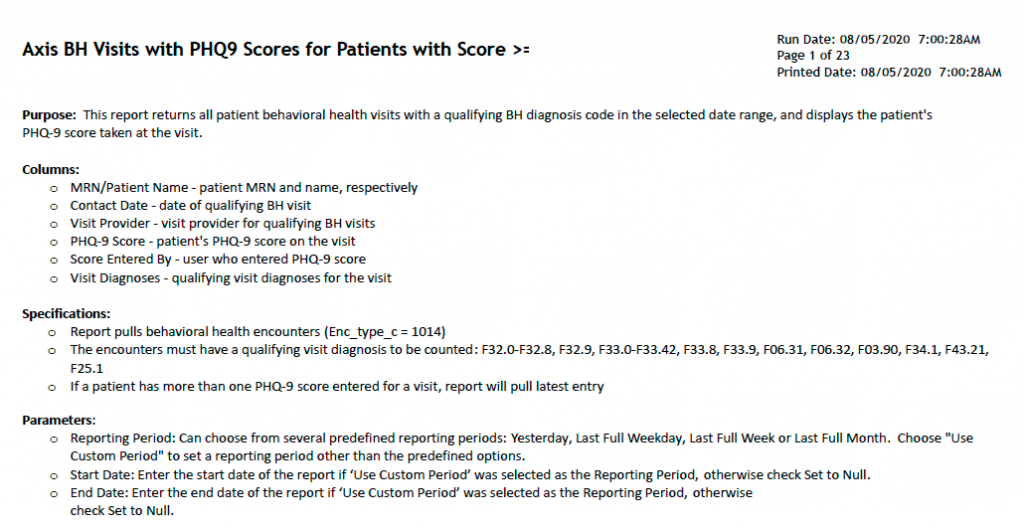
Figure 1: Example of Axis Data Registry Query
2. Examine Data in the Registry
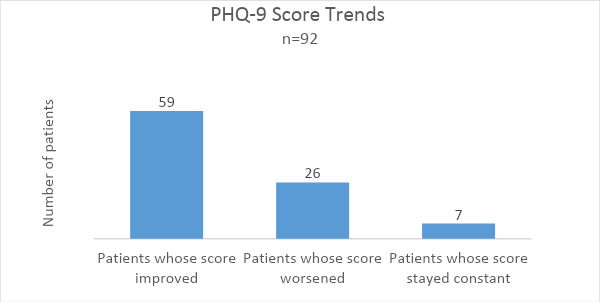
Axis analyzed patient data in the registry based on the above fields, which was beneficial since this data had not previously been available in one central location. It was particularly useful to track patients’ current medications to see which medications had been tapered on and off. With the project, Axis’ behavioral health registry report was generated automatically every month, reducing unnecessary manual repetition in sending it out. The Chief of Behavioral Health then printed the report for everyone to review as a group during monthly team meetings, rather than individually. In addition, if therapists chose to share data, patients could receive reports during appointments with behavioral health data such as their PHQ-9 trends, which empowered them to track their progress over time.

Figure 2: Example of Patient Report with Registry Data
“Data is being shared at the board level, at the senior leadership level, all the way down to the patient themselves, and that’s really cool to see.” – Amit Pabla, Chief Quality and Transformation Officer
3. Adjust Treatment
The behavioral health team had access to data from the registry that allowed them to adjust treatment based on individual changes in screening scores over time. The ICD-10 diagnosis codes tracked in the registry were used to determine if patients were eligible for additional treatment. The behavioral health team looked at data for patients who (according to their screening scores) were not improving, and referred them to psychiatrists and adjusted medication when necessary. Team members also moved patients out of treatment when they were ready to be discharged, thus freeing up space for other patients in need.
4. Measure Improvement
Axis used data from the registry to measure improvement in patients’ behavioral health screening scores based on duration of treatment and/or changes in medication. In addition to tracking individual behavioral health outcomes, Axis used the registry to evaluate its behavioral health program by looking at outcomes on a macro level. Specifically, they analyzed data by each provider across the whole behavioral health team. Results were sent to the department directors and the Chief of Behavioral Health for overall tracking. The data was also sent to behavioral health providers and the consulting psychiatrist to review specific cases during case consultation. They also monitored behavioral health provider performance based upon the data to determine where additional training might be needed.