Contra Costa Health Services had a problem. Health workers knew their safety net patients needed help with transportation, and not just to medical appointments. In this sprawling county, marked by farmland, industry and far-flung cities, people often have trouble getting to job appointments, the DMV, food pantries, the Social Security office, and other services.
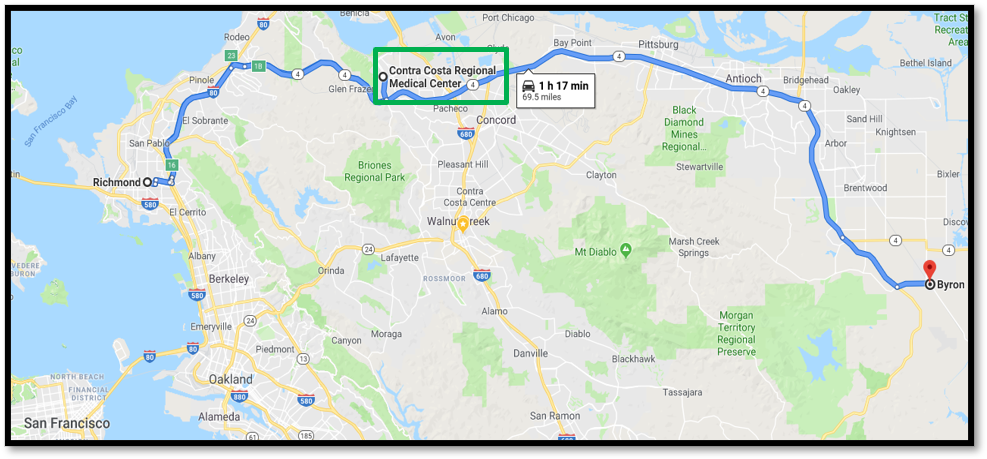
Map showing the far-flung corners of Contra Costa County. Some patients travel more than 70 miles to get to their appointments.
Under a California state initiative called Whole Person Care, a Medi-Cal waiver-funded program designed to improve the overall quality of life for people with chronic medical conditions, CCHS used voucher coupons and a fleet of taxis — the majority of them regular yellow cabs, with some “ambulance taxis” equipped for wheelchairs — to shuttle people to and from crucial non-medical appointments (See “Taxi Vouchers: Still Part of the Equation“).
As part of its Whole Person Care Pilot, the health center identifies county residents who are most likely to repeatedly go to acute care or the emergency room — something that puts a huge strain on the county health care system — and still have poor health outcomes. The pilot program goes beyond the clinic walls to connect them to the services they need. Skilled case managers meet with their clients, who are often poor, sick and isolated, to figure out unmet needs ranging from enough food to eat to a dependable way to get to work. They then set healthcare goals and coordinate treatment for physical, mental and behavioral health. This is where the taxi vouchers come in: The guidelines allow free transportation to community centers and support groups as well as school, employment, food and housing transition services, legal services, mental health care, social services and substance use treatment. (If patients need a ride to medical care, they use a different transit program.) Patients liked the taxi voucher system so much that they gave it a 4 out of 5 rating.
The issue with the taxis? Thirty-seven percent of CCHS’s safety net patients had indicated a need for this kind of transportation, but the health system was spending its entire transportation budget to serve only a fraction of them. Out of 12,500 patients enrolled in Whole Person Care, about 60 percent said their own transportation was unreliable, but just 10 percent were using the service.
In addition, the voucher program was cumbersome, with the administrative burden falling heavily on staff. Making taxi appointments for patients who requested a ride, processing vouchers, and other follow-ups took up an estimated 10 percent of 100 clinic employees’ time, leading employees to give the program a lower rating of 3.5 (“just ok”). Care coordinators would have to follow up with multiple partners when a ride fell through, and they might not find out about it until a week or two had passed. Sometimes they had to drop everything to rush a stack of paper vouchers to a patients’ homes so they could make it to a food bank and legal services the next day.
Moreover, everything was done on paper, making it all but impossible to coordinate rides across CCHS’s departments. Occasionally different departments might order the same patient multiple rides. “It could get so confusing that we once had three taxis show up to pick up the same person,” says Matt White, CCHS business intelligence officer and innovation program lead.
Finally, it often took several months to collect the invoice data needed to evaluate the effectiveness of the service. Something needed to change.