What was the problem that needed to be addressed?
Although early detection prevents progression, diabetic retinopathy is the leading cause of acquired blindness in U.S. adults. Only 10% of patients who need screening are actually screened in medically underserved populations.
What was the innovation?
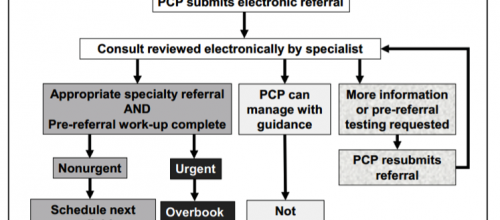
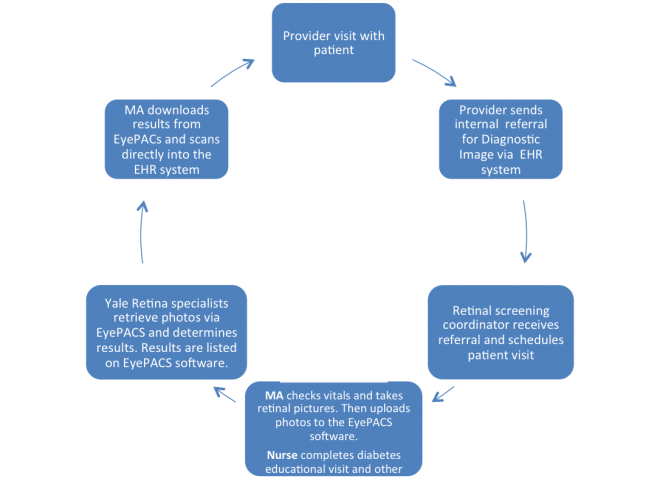
Community Health Center, Inc., a large multi-site Federally Qualified Health Center network in Connecticut, collaborated with retinal specialists at the Yale Eye Center with a primary goal to increase diabetic retinopathy (DR) screening, detection and referrals for their underserved patients. They had secondary goals to increase diabetes education, set self-management goals, reduce unnecessary referrals to eye specialists, and ensure timely referral for patients with evidence of diabetic retinopathy. They created an accessible and affordable way for their medically underserved patients to receive needed eye screening and care. Community Health Center, Inc. uses a computer software program called EyePACS to facilitate communication between a patient’s primary care provider and a retinal specialist at the Yale Eye Center. Clinic staff takes a retinal photograph of the patient and then uploads the photograph to the EyePACS program. The screening visit is coupled with a diabetes health education visit. EyePACS then alerts a Yale Ophthalmologists that a new photograph has been uploaded so that the eye specialist can review the images and provide electronic consultation to the providers regarding their patients. If needed, a patient is referred to a specialist for follow-up care.
The diabetic retinopathy screening process:
Unlike many other community health centers that absorb the costs of DR screening within the clinic, Community Health Center, Inc. has made this project sustainable by combining the screening with an educational health nursing visit. This educational visit has a checklist of items which include diabetes education, self-management goal setting, and ensuring the patient is up to date on vaccinations, foot checks, and any other testing. The educational visit is billable, allowing the clinic to keep the DR screening low-cost and accessible for their patients and clinic.
What were the results?
Within the first year, more than 550 adults were screened for diabetic retinopathy. Nearly 60% were minorities and 25% were uninsured. A total of 145 cases of DR were identified and the majority of these patients were scheduled for a one year follow-up. 75 patients were referred to a specialist. After a cost-benefit analysis was performed, each telemedicine-based DR screening was shown to cost less than conventional retinal examination ($49.95 vs $77.80). This proved to be more accessible, convenient, and affordable for all patients.
Should other practices replicate this approach?
Community Health Center, Inc. recommends this approach to be duplicated after the need has been identified. They foresee a potential challenge of recruiting retina specialists, but also know that it is not only possible to recruit specialists, but to create a long-lasting partnership for screening and follow-up care for patients. This partnership works particularly well when that group understands the “big picture and need” of the program. Making the screening visits billable has created a financially sustainable partnership and screening program for all participating groups. This screening process ran so well that Community Health Center, Inc. stated that they are “surprised at how seamless it all was” and how it is so “easily embedded into [the clinics] day”. They will continue to use this screening process in their clinics and encourage others to as well.
Additional reports and resources:
- Improving DR screening via telemedicine
- DR in Community Health
- Telemedicine vs Standard DR Evaluation
- EyePACS
Webinar
Dr.Veena Channamsetty from Community Health Center, Inc. and Dr. Tillman Farley from Salud Family Health Centers share how they’ve integrated digital retinopathy screenings into primary care at their organizations.