
Key Challenges
Communication and access to updated patient information across providers.
Q: What was the problem your organization was grappling with?
A: Many providers are widely scattered geographically in a largely rural and mountainous region, making access to care as well as access to information and communication between providers a huge challenge. Its seven larger acute-care hospitals are either non-affiliated community not-for-profit entities (three), or are part of larger hospital networks (Adventist, Dignity, and Prime). With the exception of Redding, with two larger acute-care hospitals, most urban areas are served by a single facility. Acute care in the smaller communities is provided by rural Critical Access Hospitals.
There were too many close calls and too many lengthy appointments made unnecessarily by not having real-time data. As a result, teams scrambled to coordinate care by picking up the phone to call or fax other providers and hope that patient records come.
Q: How did you learn it was a problem, and why was it important to address?
A: It was important to address this problem because so many patients have to travel to other areas and providers for care. To have the providers be able to access their patients’ records electronically, rather than relying on fax or paper carried by the patients, would make care more clinically effective, efficient, and cost effective.
Testing
Collaboration, data contribution, and achieving interoperability.
Q: Describe the solution you tested. How did you come to decide to try this solution?
A: Eight local providers and the founding members of SacValley MedShare (SVMS) recognized a community need for a health information exchange (HIE) that spanned across the rural region of Northern Central California. Hence, a health information organization (and member subscription model) called SacValley MedShare was established to facilitate health information exchange for participating provider members in the region using the technology vendor Informatics Corporation of America (ICA).
Initially, other ideas were to engage a hosted/outsourced solution, develop technology, or house technology. The solution to go with a technology vendor that housed the service for us made the most sense. This way, SVMS was not housing the data or touching the data, and the technology was already developed and proved with other HIEs.
The difficult piece was coordinating vendor proposals to find the one that would offer the most diverse range of electronic medical records (EMR) that they could work with, or have worked with, to be able to service all of our membership base. The easy piece was choosing the vendor, as others did not offer what ICA does.
Q: What structure did you put in place for the pilot (e.g. how many end users, for what use cases)? What eligibility criteria did you choose for the pilot, and why? What was the result?
A: Member provider organizations were polled to determine willingness and readiness to connect to ICA and begin contributing data. One member, an outpatient imaging group, agreed to take on the project in order to serve as a proof of concept for data contribution. They agreed to contribute thousands of anonymized imaging results to the ICA CareAlign portal. The initial test included sending anonymized imaging results via HL7 to the ICA CareAlign Exchange. This test phase lasted from April to August 2014. This test period allowed for a sufficient data sample size to be spooled into the exchange for processing. It also allowed sufficient time to analyze the data for any anomalies and determine methods for handling all of the various patient data scenarios that arise.
Through testing we learned that the CareAlign portal was capable of handling the interoperability needs of SVMS and members were impressed with the overall testing process. The data presented within the CareAlign portal was extremely useful and made patient care across the region where patients are shared easier for the patient, physician, and organizations. With a successful proof of concept in place, receiving buy-in from current and potential organizations became easier. What was difficult for member organizations, however, was finding ways to prioritize their own connectivity to ICA amongst the myriad of other IT projects that they were managing.
The next steps after the pilot was to put organizations into production. North State Radiology was the first to go live with contributing their radiology report data. The integration went well and the support from ICA kept going strong. Through constant communication and dedicated weekly technical meetings, which are still in place today, allowed the momentum to continue.
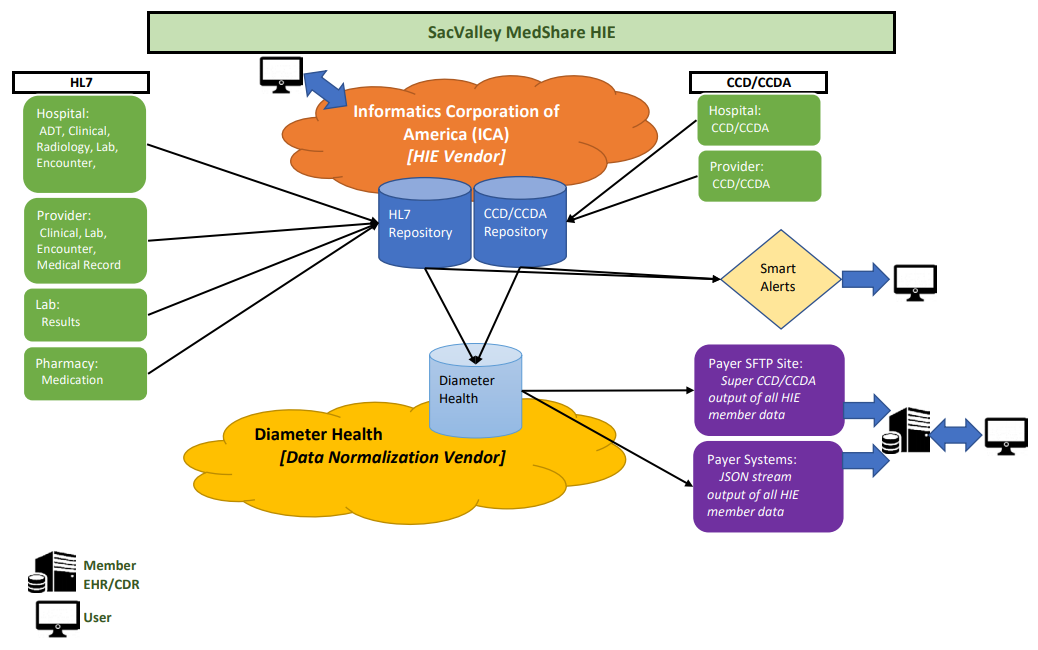
Q: How does the SVMS health information exchange work today? What services do you provide?
A: SVMS provides two main technologies to facilitate health information exchange. It provides a means for providers to securely send medical information to one another, rather than relying on fax or mail. This is called Direct Secure Messaging, or “Direct.” It also provides a platform where participants can securely make real-time data available to other participants via the web or integrated EMR exchange, as well as rapidly search for information on a patient that they are treating from all of the participants. That is called “Exchange,” including medications, allergies, labs, radiology reports, and diagnoses.
Other features include SmartAlerts®, which provide real-time alerts or a daily digest file for health insurers, members, or county agencies on their patients when they have an encounter at a participating member facility.
In addition to providing the technology for enhancing communication, SVMS provides a key forum for active exchange of ideas and non-patient information between participants who previously had exchanged very little between themselves.
Lessons & Next Steps
Competition, financial sustainability, and population health analytics.
Q: What are some of the key insights and learnings from your experience implementing an HIE?
A: The technology is the easy part; the political part is the tougher piece. Hospitals are often in competition with other hospitals — their referral patterns overlap and time has made them more adversarial than collaborative. It took a while to get them to the table to invest and put patients benefits first. Sometimes they only look at the price tag before they see the value.
In addition, independent providers and medical associations are not as organized or enthusiastic as we would have hoped. Perhaps there needs to be more education and understanding the barriers — if they’re technology adverse, content with status quo, or something else.
Most importantly, the financial sustainability model that we’ve built for participating members should be borrowed. SVMS was initially incubated by the Hospital Council in 2012, then became an independent not-for-profit in 2013, and was financially self-sustainable by 2015. We have a subscription model (quarterly dues) for hospitals based on number of beds and outpatient facilities based on number of providers. The pricing strategy was based on what we could charge that would be reasonable and affordable for participating members, while also being able to pay for the HIE vendor. In addition, we have two full-time employees and built in cash reserves to sustain those employees.
Q: What is next for your team? Are you planning to expand the solution to other providers and patient populations?
A: We’re currently looking into grant funding for a data analytics platform. We’ve looked at three vendors and have the average cost. The platform would allow you to drill down for population health and public health “hot spots” and help with MIPS reporting (CMS mandated reporting, such as areas across counties that have the most diabetics). Kansas Health Information Network is doing this and turning around and selling it as a product.
We now 320,000 lives in our Master Patient Index, and our population service area is 880,000. By the end of next year, we’ll have more than half in the Master Patient Index. Trying to get to 100 percent saturation is challenging.


