In December, seven participants and program team members from Kaiser Permanente’s cardiovascular disease risk reduction initiatives attended a site visit at Livingston Health Center in California’s Central Valley.
Here, we learned about the components of Livingston’s successful pilot program for self-measured blood pressure (SMBP) control — from the strategic commitment to quality improvement that spawned it, to the health coaching and education program that enhanced it, to the data analytics that support it. Our group heard from several members of the multidisciplinary team that carries out the program, ranging from the c-suite to the care and education providers that engage directly with patients. We toured Livingston’s beautiful new facility, watched an SMBP visit demonstration, and came away brimming with ideas. All were grateful for the materials and lessons that were shared by the team, and to Dr. Chetan Gujarathi, for co-creating and facilitating such a productive site visit.
Planning and Piloting SMBP
Livingston began its participation in the PHASE program in 2016 as part of a learning collaborative designed to improve data driven decision-making. In November 2017, Livingston’s PHASE team attended the bi-annual grantee learning community convening and learned about the self-measured blood pressure (SMBP) intervention from Dr. Mike Rakotz of the American Heart Association. SMBP, also known as home blood pressure monitoring or out-of-office blood pressure measurement, has been shown to be an effective approach to lower BP and improve control among patients with hypertension. In 2017, the American College of Cardiology, the American Heart Association and others issued a new clinical practice guideline for hypertension which recommends out-of-office blood pressure measurement to confirm diagnosis of hypertension and for medication titration (in conjunction with telehealth counseling or other interventions) and effectively increasing patient engagement.
The Livingston team was inspired and excited about the possibility for improved hypertension control among their patients and initiated a planning process to determine how they might use this intervention with their patients. While SMBP is often used to confirm a hypertension diagnosis, Livingston instead used it to target their highest risk patients, defined as those patients 40 – 64 years old whose last blood pressure reading was greater than or equal to 160/90 within the last 12 months. By offering the SMBP intervention to these patients, they hoped to not only reduce risk of heart attack and/or stroke by lowering their blood pressure but also hoped to put them on a pathway to engaging them with their health and self care for the long run.
Fatima Jaimes, Livingston’s director of nursing, described the planning process and the critical success factors for launching the pilot. They include:
- Leadership buy in.
- Multidisciplinary collaboration and team-based approach. Livingston’s program involves nurses, care coordinators, health educators, and providers.
- Frequent, regular communication, such as weekly team meetings and program monitoring check-ins.
- Effective use of HIT and data analysis, which includes:
- Using i2iTracks to create a registry of patients meeting the inclusion criteria at its Delhi Health Center site.
- Building an appointment template in their electronic health record, NextGen, for care coordinators and/or nurses to schedule appointments directly.
- Developing training materials for both for patients and staff, (note: Livingston utilized the TargetBP materials from the AMA/ACA), developing telephone scripts, and health coach training. (All of Livingston’s RNs are trained health coaches.)
- Utilizing grants to purchase blood pressure cuffs.
Livingston’s program design consists of an initial visit where patients learn to use the blood pressure cuff and log their blood pressure twice per day for 1 week. Check ins continue with a one-week follow up, one-month follow up, two-month follow up and six-month follow up.
The initial visit is critical; it’s a great opportunity to engage intensively with a patient. The staff quickly realized that while their planned 30-minute visit might be sufficient for teaching about the blood pressure cuff, they were missing the opportunity to do much more. For this reason, the initial visit was increased to an hour so that medication reconciliation and health coaching could be included in the visit.
At the one-week follow up visit, patients return the cuffs and turn in their log. Blood pressure readings for the week are verified and scanned into NextGen, Livingston’s electronic health record. Nurses report that this visit – and the power of the data – can be especially influential in building a patient’s activation and engagement.
Over the course of six months, health education and coaching continues at each follow up visit, and patients are encouraged and supported to take small steps and set goals for healthier eating, smoking cessation, increased exercise, etc. Often they work with a care coordinator and are given a referral to Livingston’s Health Education Department.
The results of the pilot program were very encouraging, especially considering the high-risk population of focus:
# |
% |
|
| Number of patients eligible at target site | 35 | |
| Number of patients called | 35 | 100% |
| Number of patients successfully scheduled for SMBP program | 9 | 26% |
| Number of appointments kept | 9/9 | 100% |
| Number of patients with improved med list after reconciliation | 4/9 | 45% |
| Number of patients with improved blood pressure readings after SMBP | 8/9 | 89% |
| Number of patients with blood pressure readings at or below control | 2/9 | 22% |
Livingston is now training additional nurses and spreading the program to other clinical sites.
A Culture of Quality
Chief Medical Officer Dr. Glen Villanueva and Chief Operating Officer Feras Khoury joined our site visit to provide the strategic leadership perspectives from which the SMBP program grew.
Dr. Villanueva described the QI principles and practices he introduced since his arrival at Livingston Health Center in November, 2018. Noting that QI programs can sometimes be a “check the box” endeavor, Dr. Villanueva sought to move from a process that changed priority each month (which is not often conducive to sustained improvements) to a more focused approach on four key conditions: hypertension, diabetes, adult obesity, and pediatric obesity. He noted that quality improvement can seem punitive to providers — “here are all the things you’re not doing” — and wanted to change that perception as well. The tenor was shifted to presenting data in a non-threatening way (blinded and confidentially at first) so that finding and sharing best practices could become the focus.
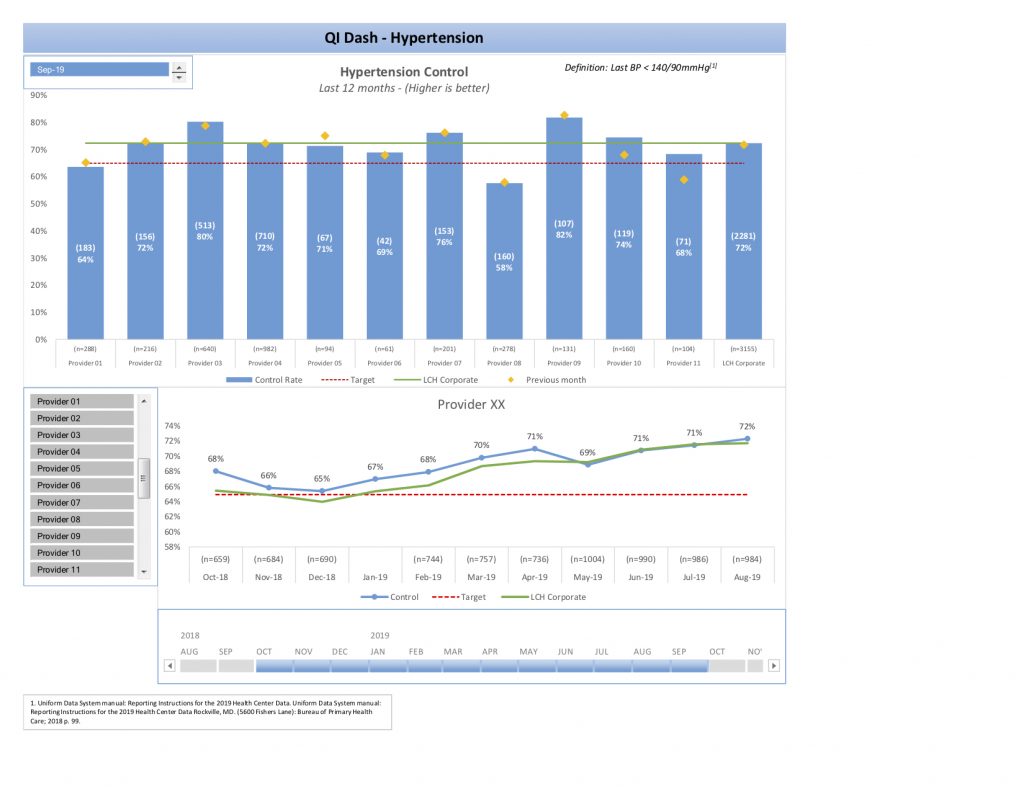
Livingston has seen remarkable improvement in hypertension control over the past year and a half:
- In Q1 2018, their control rate was 56 percent among approximately 2,100 patients in the population of focus and they set a target of 5 percent improvement.
- By Q3 2019, their control rate was 70 percent among approximately 3,100 patients in the population of focus. This represented an 11 percent absolute and 20 percent relative improvement rate.
Dr. Villanueva identified many components that contribute to building a culture of clinical excellence: educating providers, training medical assistants on taking accurate blood pressure, RNs establishing the SMBP program, extensive health education efforts, outreach, follow up, and assessing missed opportunities for care. During this time Livingston also formally established a Health Education Department, with increased staffing of four additional full-time Wellness Coordinators, to provide supportive services. Now Livingston offers regular diabetes education classes, nutrition education, help with smoking cessation and generally more capacity for these important services.
Naturally, our thoughts turned to the fiscal effect of providing these nurse visits and support services, which are mostly non-billable. However, we learned there are factors beyond reimbursable visits to consider when estimating the return-on-investment for building a culture of quality and providing enabling services. While Livingston does receive some quality incentives and grants they’ve found that as their focus on quality and outcomes increased, physician and staff turnover has decreased and use of locums tenens has all but ceased. Patient visits have increased, mostly through family and friend referrals, and Livingston Health Center has become a desired place of employment in the area.
Building Data Capacities
Our final exploration of the day focused on building the data capacities illustrated below.
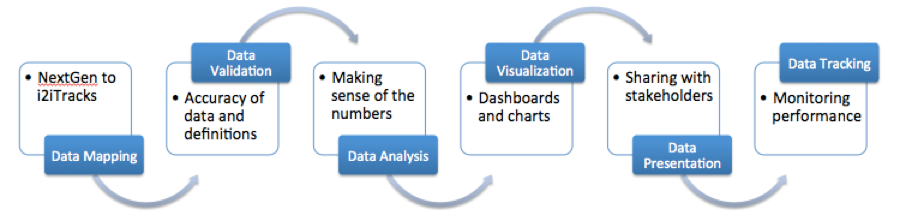
We all know that accurate, complete, and timely data is essential for measuring performance and improvements, but at Livingston they’ve found that equally important is how that data is communicated. To be “consumable” and actionable, performance measures and outcomes measures should be presented to providers and staff by their department head or supervisor — not by QI, IT, or data analysts. Livingston’s QI team and department heads work together to validate data and build self-service dashboards, thus ensuring their improvements are driven by and monitored with data and embodying Demming’s famous observation, “Without data you’re just another person with an opinion.”
Find this useful or interesting? We’re constantly sharing stuff like this. Sign up to receive our newsletter to stay in the loop.